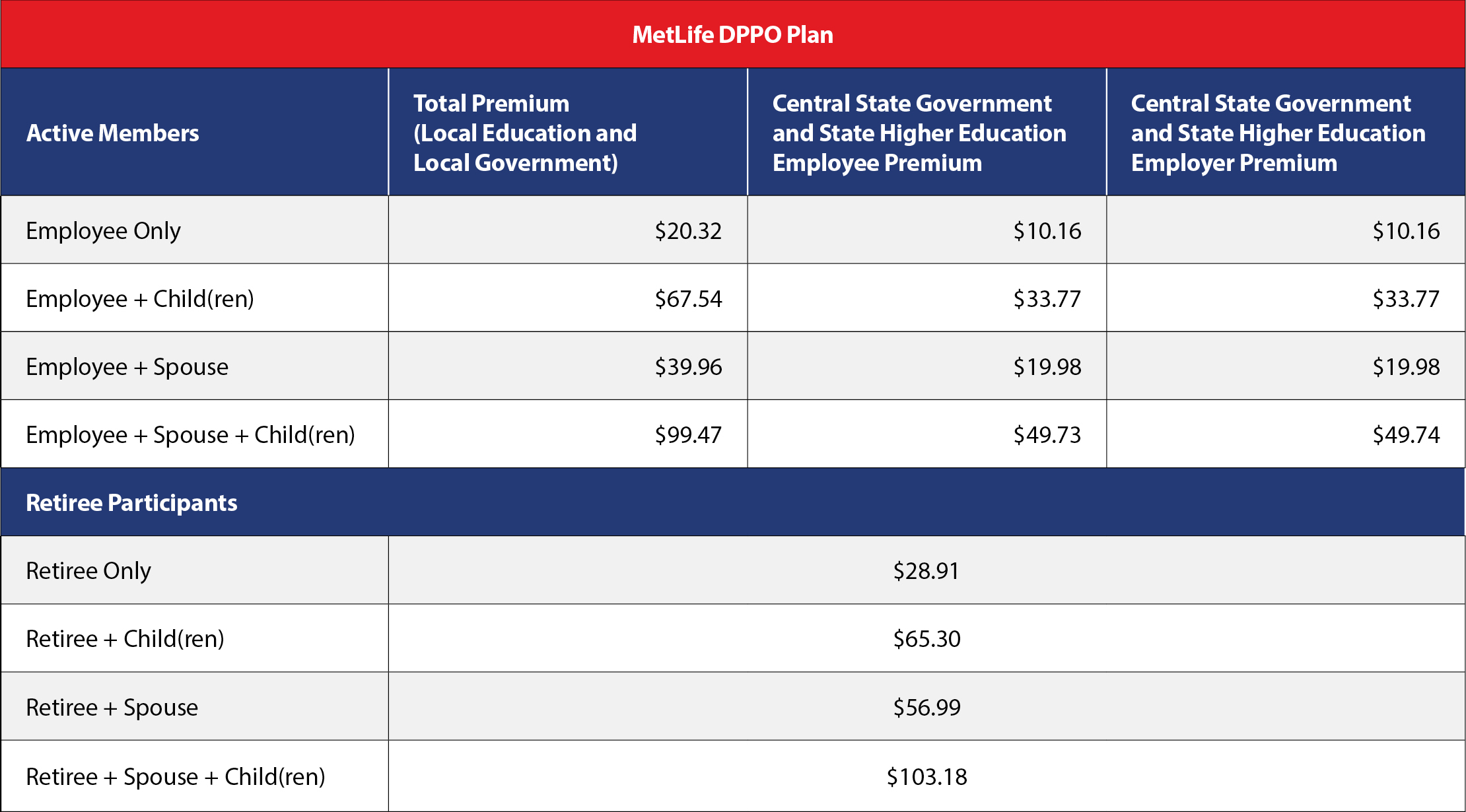
Rates
Rates
DENTAL INSURANCE: EXCLUSIONS
We will not pay Dental Insurance benefits for charges incurred for:
1. services which are not Dentally Necessary, or those which do not meet generally accepted standards of care for treating the particular dental condition;
2. services for which You would not be required to pay in the absence of Dental Insurance;
3. services or supplies received by You or Your Dependent before the Dental Insurance starts for that person;
4. services which are neither performed nor prescribed by a Dentist, except for those services of a licensed Dental Hygienist which are supervised and billed by a Dentist, and which are for:
- scaling and polishing of teeth; or
- fluoride treatments;
5. services which are primarily cosmetic, unless required for the treatment or correction of a congenital defect of a newborn Child;
6. services or appliances which restore or alter occlusion or vertical dimension;
7. restoration of tooth structure damaged by attrition, abrasion or erosion, unless caused by disease;
8. restorations or appliances used for the purpose of periodontal splinting;
9. counseling or instruction about oral hygiene, plaque control, nutrition and tobacco;
10. personal supplies or devices including, but not limited to: water piks, toothbrushes, or dental floss;
11. decoration or inscription of any tooth, device, appliance, crown or other dental work;
12. missed appointments;
13. services:
- covered under any workers’ compensation or occupational disease law;
- covered under any employer liability law;
- for which the Employer of the person receiving such services is required to pay; or
- received at a facility maintained by the Policyholder, labor union, mutual benefit association, or VA hospital;
14. services covered under other coverage provided by the Policyholder;
15. temporary or provisional restorations;
16. temporary or provisional appliances;
17. prescription drugs;
18. services for which the submitted documentation indicates a poor prognosis;
19. the following, when charged by the Dentist on a separate basis:
- claim form completion;
- infection control, such as gloves, masks, and sterilization of supplies; or
- local anesthesia, non-intravenous conscious sedation or analgesia, such as nitrous oxide;
20. dental services arising out of accidental injury to the teeth and supporting structures, except for injuries to the teeth due to chewing or biting of food;
21. caries susceptibility tests;
22. appliances or treatment for bruxism (grinding teeth);
23. precision attachments associated with fixed and removable prostheses, except when the precision attachment is related to implant prosthetics;
24. adjustment of a Denture made within 6 months after installation by the same Dentist who installed it;
25. duplicate prosthetic devices or appliances;
26. replacement of a lost or stolen appliance, Cast Restoration or Denture;
27. replacement of an orthodontic device;
28. diagnosis and treatment of temporomandibular joint disorders and cone beam imaging associated with the treatment of temporomandibular joint disorders;
29. intra and extraoral photographic images;
30. adult prophylaxis for Dependents under age 14.